dr. harry landrum, optometric physician contact lens care agreement contact lenses are fda class 1 medical devices that have the pot
Dr. Harry Landrum, Optometric Physician
CONTACT LENS CARE AGREEMENT
Contact lenses are FDA class 1 medical devices that have the potential
for serious complications if not used and fitted properly. For that
reason, the standard of care and the requirements of the New Jersey
State Board of Optometry and the federal government require an annual
examination for the renewal of a contact lens prescription. In
addition to general eye health assessment, the doctor will assess
issues related to contacts such as abnormal blood vessel growth,
corneal damage, chronic inflammation, hygiene, discomfort and poor
surface compatibility, in addition to vision changes. The estimated
fee for these services range between $85 and $155. These fees will
cover contact lens related follow ups for a 30 day period. If you
cannot complete the fitting procedure in the allotted time due to
missed follow up appointments, there will be an additional $35 charge
per visit beyond the global time period. Additional fees for training
for insertion and removal of contact lenses is approximately $70 to
all new wearers.
By signing, I acknowledge that I understand the policies regarding the
fitting of contact lenses and agree to the associated fees. I
understand that these fees are an estimate and are subject to changes
based on the doctor's final assessment. I also understand that
improper usage of contact lenses as prescribed can lead to vision loss
and permanent eye damage. I understand that if an infection is
present, I will need to be treated under my medical insurance prior to
being refit with contact lenses.
Signature:_____________________________________________________
Date:_______________________
CONTACT LENS QUESTIONNAIRE
1. What brand of contacts are you now wearing, if any?
_____________________________________________
2. Do you experience dryness with your contact lenses?
_____________________________________________
3. Have you had a contact lens related eye infection or complication?
__________________________________
If so, please describe
__________________________________________________________________
When?
_____________________________________________________________________________
4. Have your eyes become contact lens intolerant over the years?
_____________________________________
5. How often do you change your contact lenses?
__________________________________________________
6. Can you see distance comfortably with your contacts?
____________________________________________
7. Can you see near comfortably with your contacts?
_______________________________________________
8. How many days a week do you wear your contacts?
_____________________________________________
9. How many hours a day do you wear your contacts?
______________________________________________
10. Do you sleep in you contact lenses?
_________________________________________________________
11. If you sleep in your contacts, for how many nights in a row?
_____________________________________
12. What solutions are you currently using, if any?
________________________________________________
13. Do you rub your contact lenses with solution when cleaning?
_____________________________________
14. If you store your lenses in solution, do you discard your solution
every morning?
_________________________________________________________________________________________
15. How often to you change your contact lens case?
______________________________________________
16. Do you have a backup pair of eyeglasses?
____________________________________________________
Please rank 1- most important to 4 - least important:
_____Convenience _____Comfort _____Clarity _____Cost
 INSTITUTO SALVADOREÑO DEL SEGURO SOCIAL DEPARTAMENTO DE CIRUGIA NOVIEMBRE
INSTITUTO SALVADOREÑO DEL SEGURO SOCIAL DEPARTAMENTO DE CIRUGIA NOVIEMBRE SEÑOR GUILLERMO LARRAÍN RÍOS SUPERINTENDENTE DE VALORES Y SEGUROS
SEÑOR GUILLERMO LARRAÍN RÍOS SUPERINTENDENTE DE VALORES Y SEGUROS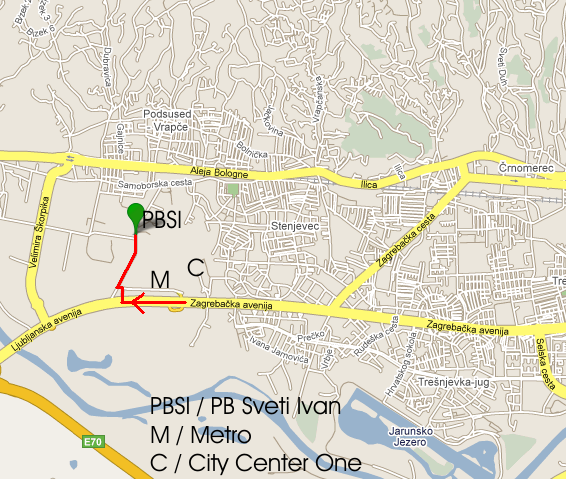 KAKO DOĆI DO PSIHIJATRIJSKE BOLNICE „SVETI IVAN“? AUTOBUSOM
KAKO DOĆI DO PSIHIJATRIJSKE BOLNICE „SVETI IVAN“? AUTOBUSOM  DISPOSITIVO DE TRÁFICO DURANTE “LA NOCHE TOLEDANA” EDICIONES DE
DISPOSITIVO DE TRÁFICO DURANTE “LA NOCHE TOLEDANA” EDICIONES DE WITAJCIE NA LEKCJI WYCHOWANIA FIZYCZNEGO! (27042020) TEMAT LEKCJI KOSZYKÓWKA
WITAJCIE NA LEKCJI WYCHOWANIA FIZYCZNEGO! (27042020) TEMAT LEKCJI KOSZYKÓWKA C 3 DE FEBRERO DE 2020 1 EXPOSICIÓN PARA
C 3 DE FEBRERO DE 2020 1 EXPOSICIÓN PARA VERSION NUMBER 13 DATE DECEMBER 2016 ONLINE 3G PLEXTOR
VERSION NUMBER 13 DATE DECEMBER 2016 ONLINE 3G PLEXTOR EL PATRIMONIO CULTURAL OBJETIVO AMPLIAR TUS APRENDIZAJES ACERCA DEL
EL PATRIMONIO CULTURAL OBJETIVO AMPLIAR TUS APRENDIZAJES ACERCA DEL VOTOS Y BANCAS LA REPRESENTACIÓN PROPORCIONAL EN TIERRA DEL
VOTOS Y BANCAS LA REPRESENTACIÓN PROPORCIONAL EN TIERRA DEL P AŃSTWOWA SZKOŁA MUZYCZNA I I II ST IMIJPADEREWSKIEGO
P AŃSTWOWA SZKOŁA MUZYCZNA I I II ST IMIJPADEREWSKIEGO IGRE UZ POŠTOVANJE MJERA „U DJEČJOJ IGRI ČESTO JE
IGRE UZ POŠTOVANJE MJERA „U DJEČJOJ IGRI ČESTO JE INSTRUCTIVO PARA EL LLENADO DE LOS FORMULARIOS DE DESCRIPCIÓN
INSTRUCTIVO PARA EL LLENADO DE LOS FORMULARIOS DE DESCRIPCIÓN I IZMJENE FINANCIJSKOG PLANA I GODIŠNJEG PROGRAMA GRAĐENJA I
I IZMJENE FINANCIJSKOG PLANA I GODIŠNJEG PROGRAMA GRAĐENJA I