work experience and work placement application form strictly confidential your details name: date of birth: age o
Work Experience and Work Placement
Application Form
STRICTLY CONFIDENTIAL
YOUR DETAILS
Name:
Date of Birth:
Age on first day of placement:
Home address:
Post code:
Mobile:
Home number:
Email address:
Emergency contact name:
Emergency contact number:
SCHOOL/UNIVERSITY DETAILS
School/College/University:
Address:
Post code:
Phone number:
Teacher/Tutor name:
Teacher/Tutor phone number:
Teacher/Tutor email address:
PLACEMENT DETAILS
Dates work experience placement required:
Qualifications held and/or being studied:
Area you are interested in for work experience:
(please note not all departments are able to host work experience due
to the nature of the work, and due to high demand you may not always
be able to be placed within your preferred area)
SUPPORTING INFORMATION
Please use this space to describe what skills/abilities you possess
that would make you suited to the area of work you have requested for
your placement:
Please indicate any disabilities or health problems, which the Trust
might have to make special arrangements to accommodate:
REHABILITATION OF OFFENDERS ACT 1974-amendments order 2002
(IF APPLICANT OVER 18)
The National Health Service is exempt from the provisions of Section 4
(2) of the Rehabilitation of Offenders Act. Under this act you must
therefore declare any criminal convictions, even if they are “spent”
received either prior to your application for a Work Placement or
during it. Failure to disclose such convictions may result in the
immediate termination of your work placement.
If appropriate, please state “no convictions to declare”
(or please provide relevant information of convictions below)
Signed: Date:
CONFIDENTIALITY
Anyone undertaking a Work Placement in the Countess of Chester
Hospital NHS Foundation Trust is likely to become aware of, and have
access to, confidential information about patients, staff, members of
the public and health service business.
The very fact that a person is receiving treatment or attending for a
consultation is itself a confidential matter and he/she has the right
to expect that their privacy is protected.
On no account, therefore, must any information relating to
identifiable individuals be divulged to anyone other than authorised
persons e.g. medical, nursing or other professional staff as
appropriate, who are concerned directly with the care, diagnosis and /
or treatment of the patient.
If you are in any doubt as to the authority of a person or body asking
for information of this nature, you must seek advice from the senior
person on the ward or the department to which you are attached.
Any breach of this obligation to observe confidentiality and Data
Protection will result in immediate termination of your Work
Placement-
DATA PROTECTION ACT 1998
The Trust collects stores and processes personal data about students
on placement for the purpose of administering and managing the
placement and educational program and all other services provided by
the Trust. Information may be disclosed to your organisational sponsor
or relevant organisations where necessary for the fulfillment of the
Trusts legal obligations.
Please read the following statement and sign the declaration below:
As the individual named below, I have read and understood the Trust’s
statement “Confidentiality during Work Placement” and agree to be
bound by its terms. I undertake not to disclose information learnt in
the course of my presence in the Trust to anybody outside the Trust.
If I feel disclosure is necessary in the public, patient or family
interest, I will discuss this with the appropriate health professional
or senior manager.
I understand that a breach of this obligation may result in my work
placement being terminated and that other action may be taken against
me.
Signed: Date:
Print name:
FOR STUDENTS UNDER 18 YEARS ONLY:
As parent/guardian of the aforementioned work placement student, I
agree to my child undertaking a work experience placement and he / she
will observe the conditions set out above. I confirm that I will
inform the Trust of any medical condition that would prevent my child
from undertaking the placement.
Signed: Date:
(Parent/Guardian – please delete as necessary)
Please be aware there is a currently a high demand for work experience
placements therefore you may not receive a response straight away. We
aim to provide a response within approximately 4 weeks.
Thank you for completing the application form, please return to:
Learning and Development, Education and Training Centre, Countess of
Chester Hospital NHS Foundation Trust, Liverpool Road, Chester CH2 1UL
Tel: (01244) 365834
Equal Opportunities Monitoring Form
The Countess of Chester Hospital NHS Foundation Trust is committed to
ensuring that applicants are considered for a placement irrespective
of gender, sexual orientation, marital or parental status, disability,
religion, social class, nationality or ethnic origin.
In order to monitor the effectiveness of our Equal Opportunities
Policy, we require applicants to provide the information outlined
below. This information is confidential and used solely for monitoring
purposes. Such use will be subject to the provision of the Data
Protection Act 1998.
1. Personal information
Title
Surname
First names
Date of birth
2. Ethnic Origin (UK applicants only). I would describe myself as:
□
White
□
Other Asian background
□
Gypsy or Traveller
□
Arab
□
Black or Black British – Caribbean
□
Mixed – White and Black Caribbean
□
Black or Black British – African
□
Mixed – White and Black African
□
Other Black background
□
Mixed – White and Asian
□
Chinese
□
Other Mixed background
□
Asian or Asian British - Pakistani
□
Other Ethnic Background
□
Asian or Asian British - Bangladeshi
□
Not known
□
Asian or Asian British - Indian
□
Information refused
3. Disability. I would describe myself as:
□
No disability
□
Social/communication impairment such as Asperger’s syndrome/other
autistic spectrum disorder
□
Blind or have a serious visual impairment uncorrected by glasses
□
Deaf or a serious hearing impairment
□
A long standing illness or health condition such as cancer, HIV
diabetes, chronic heart disease or epilepsy
□
A mental health condition such as depression, schizophrenia or anxiety
disorder
□
A specific learning difficulty such as dyslexia, dyspraxia or AD(H)D
□
A physical impairment or mobility issue such as difficulty using arms
or using a wheelchair or crutches
□
A disability, impairment or medical condition that is not listed
□
Two or more impairments and/or disabling medical conditions
Please list any reasonable adjustments you think you may require:
 MÁS DE 150 PERSONAS DEBATEN SOBRE LA SITUACIÓN DEL
MÁS DE 150 PERSONAS DEBATEN SOBRE LA SITUACIÓN DEL S OLICITUD DE ADMISIÓN SOCIOA TITULAR (60€) SOCIOA ADHERIDO1
S OLICITUD DE ADMISIÓN SOCIOA TITULAR (60€) SOCIOA ADHERIDO1 FUNDACION PARA LA INVESTIGACIÓN BIOMÉDICA HOSPITAL GREGORIO MARAÑÓN MADRID
FUNDACION PARA LA INVESTIGACIÓN BIOMÉDICA HOSPITAL GREGORIO MARAÑÓN MADRID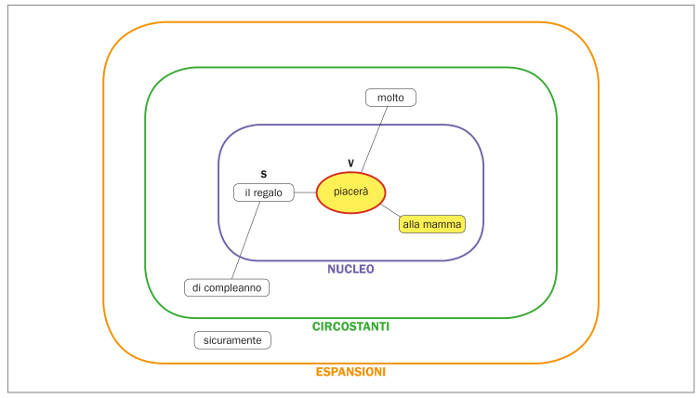 DECALOGO DELLA GRAMMATICA VALENZIALE PER PUNTI 1 IL MODELLO
DECALOGO DELLA GRAMMATICA VALENZIALE PER PUNTI 1 IL MODELLO F IRST SERBIAN (26TH YU) CONGRESS ON THEORETICAL AND
F IRST SERBIAN (26TH YU) CONGRESS ON THEORETICAL AND RD N° 3252012 MONTEVIDEO 3 DE OCTUBRE DE 2012
RD N° 3252012 MONTEVIDEO 3 DE OCTUBRE DE 2012 ACCESIBILIDAD EN LOS PORTALES WEB DE LAS COMUNIDADES AUTÓNOMAS
ACCESIBILIDAD EN LOS PORTALES WEB DE LAS COMUNIDADES AUTÓNOMAS FEBRUARY 2020 FREEDOM OF INFORMATION ACT (FOIA) REQUEST –
FEBRUARY 2020 FREEDOM OF INFORMATION ACT (FOIA) REQUEST –