rodent surgery recommendations for the performance of rodent surgery are based on the 1996 edition of the nih guide for the care and use o
Rodent Surgery
Recommendations for the performance of rodent surgery are based on the
1996 edition of the NIH Guide for the Care and Use of Laboratory
Animals and 9 CFR, the Animal Welfare Act (AWA). Part 2 of the AWA
states that major surgical procedures on rodents "must be performed
using aseptic procedures." Adequate procedures include the use of
sterile instruments, sterile surgical gloves, and aseptic preparation
of the surgical site in order to prevent postoperative infections. A
separate facility for rodent surgery is not necessary. A rodent
surgical area can be a room or portion of a room that is easily
sanitized and not used for any other purpose during the time of the
surgery.
Rodents include hamsters, gerbils and guinea pigs, as well as rats and
mice. Guinea pigs and hamsters are USDA covered species, meaning that
they are not exempt from USDA regulations and the provisions of the
AWA. Rodent surgery can be classified as minor or major in nature.
Anesthesia and anesthetic agents of rodents will not be discussed
here. One should not overlook the utility of local anesthetics. Please
contact one the Department’s veterinarians for more information
concerning the use of various anesthetics, analgesics, and
tranquilizers. General information concerning various anesthesia,
analgesia, and tranquilization agents can be found in the "Anesthesia,
Analgesia, and Tranquilization Guidelines." Paralytic agents may not
be used without anesthesia. To prevent corneal desiccation, place
ophthalmic ointment in both eyes of rodents undergoing anesthetic
procedures. The administration of antibiotics and analgesics prior to
commencing a procedure can make them more effective.
Surgical procedures can be divided into two main groups—survival and
nonsurvival. Further subdivisions of survival procedures are made with
regard to whether the procedure(s) involves penetrating a body cavity
or causing physical impairment. Procedures penetrating a body cavity
and/or causing physical impairment are termed major survival surgical
procedures, procedures which do not are termed minor survival surgical
procedures. Multiple major survival surgical procedures are not
permitted on animals without scientific justification.
Minor Surgery
"Minor survival surgery is defined as any procedure which does not
expose a body cavity and causes little or no physical impairment" (the
"Guide," p 63) and includes injections, venipuncture, and subcutaneous
implants. When conducted with proper care, these techniques present
few difficulties. "Minor procedures are often performed under less
stringent conditions than major procedures but still require aseptic
technique and instruments and appropriate anesthesia." (the "Guide," p
62) Be aware that much rodent research is performed within human
medical centers and that implants or instruments can contaminate
rodents with human pathogens if improper technique is used.
Major Surgery
Major surgery includes invasion of the cranial, abdominal, or thoracic
cavities. Any procedure that might leave the rodent with a permanent
handicap, whether physical or physiological, would also be considered
major surgery. The use of aseptic technique is mandatory in these
surgeries to minimize the possibility of postsurgical infection.
Consultation with one of the Department’s veterinarian is recommended
if you have questions regarding techniques appropriate for these
situations.
Chronic Implants
Chronic implants, such as chronic intravenous catheters and head caps,
are intermediate in nature, but are techniques presenting the most
severe postsurgical infections, at least in the cases presented to
UNTHSC’s DLAM. Surgical technique needs to be meticulous, as for major
surgery. Postsurgically, use sterile technique when accessing the
catheter (s). The most critical requirement is to inject only sterile
solutions into the catheter. Solutions should be freshly prepared or
stored under refrigeration if prepared in advance. The top of the vial
or mouth of the container containing solutions for injection must be
kept clean and wiped with alcohol or flamed before drawing up the
solution. Inoculation of even a few organisms into an intravenous
catheter may result in death of the animal due to sepsis.
General Guidelines
The location of the area used for major rodent surgery is not critical
but should be located in a portion of the laboratory that is not
heavily traveled. (Please note: An investigator’s laboratory may be
used as a rodent survival surgery area provided such use is approved
and certified by the ARC.) The surgical "table" must be constructed of
a material that can be washed with soap and water and then disinfected
using appropriate agents (see attached Table 1) or that can be heat
sterilized. The immediate surgical area should be disinfected prior to
and between surgeries to decrease dust borne contamination and should
not be used for other purposes during the time of surgery.
Surgical instruments must be sterile. Heat sterilization is ideal.
Agents such as chlorine dioxide or gluteraldehydes can be used for
cold sterilization. Chlorine dioxide is not documented as being toxic
to animal tissue but will corrode stainless steel instruments.
Gluteraldehyde must be thoroughly rinsed off of instruments with
sterile saline or water before use of delicate items, such as drills
and burrs. Disinfectants should be replaced when contaminated with
blood or other body fluids. Catheters and implants can be sterilized
using ionizing radiation or ethylene oxide (see attached Table 2).
Performing pre-surgical evaluations help insure your prospective
patients are not overtly ill. Is the animal alert with a smooth coat
and clear eyes? Withholding food is not necessary in rodents unless
specifically mandated by the protocol or surgical procedure. Water
should NOT be withheld unless required by the protocol. Withholding
food for more than six hours should be discussed with a veterinarian.
Preparation of the animal should include clipping or shaving the
surgical site with a generous border (at least 1 cm) to keep hair from
contaminating the incision (hair removal should be performed in a
location remote from the surgical area). The surgical site should be
scrubbed with a germicidal scrub (see attached Table 3), being careful
to scrub from the center of the site toward the periphery. The site
can then be rinsed with a 70% alcohol, sterile water, or sterile
saline. Three alternating preps of germicidal scrub and rinse are
considered adequate. Note that alcohol will also contribute to
hypothermia if liberally used. Finally, the area should be draped with
sterile drapes, which not only helps prevent stray hair from entering
the surgical field, but also provides a sterile area on which to lay
sterile instruments during surgery.
The surgeon must thoroughly scrub his or her hands with a bactericidal
scrub (see attached Table 3). The use of sterile surgical gloves is
necessary. A surgical mask should be worn for major surgeries. Wearing
a clean lab coat is mandatory. A sterile gown is preferable for major
surgeries.
Surgical instruments, gloves and other paraphernalia may be used on
more than one animal. Any item used on multiple animals must be
carefully cleaned and disinfected between animals (see attached Table
4). Alternating two or more sets of instruments is one way to allow
time for instruments to sit in a disinfectant or sterilant solution
for more than just a few minutes.
Animal evaluation during surgery is critical. Monitoring of anesthetic
depth is usually of first importance. Unfortunately, techniques for
monitoring anesthetic depth vary somewhat with the agent used. A quiet
animal that does not move when a painful stimulus is applied is the
most certain indicator of adequate anesthesia, however, the zone
between quiet and too quiet is very narrow in rodents.
Maintaining body temperature is next in importance, as anesthetics
induce hypothermia either directly or indirectly. It is easier to keep
animals warm than warm them up. Warm water blankets or bottles provide
supplementary warmth without being too hot. Bubble wrap helps small
rodents maintain body temperature. During surgeries, warm sterile
fluids (saline or lactated Ringers solution) should be provided. These
can be administered subcutaneously, intravenously or
intraperitoneally. Any tissues exposed for long periods during surgery
should be kept moist with these same warmed solutions. Some anesthetic
agents, such as xylazine, will predispose an animal to volume
depletion.
Observation during postsurgical recovery is important. The animal, in
or out of its cage, must be kept warm. Warm water pads, bubble wrap,
blankets, or the blue "diaper" pads work well. The use of electric
heat pads or heat lamps may overheat the animal; their use is
discouraged. If electric heat pads or heat lamps must be used,
provision must be made to make frequent observations and turning of a
somnolent animal so that the animal will not be overheated, with
preventing burns being of the utmost importance. Provision must also
be made so that an awake animal can escape the heat source when it
becomes too warm. Warmed fluids can be administered subcutaneously,
intravenously, or intraperitoneally if there is any suspicion the
animal may be dehydrated. Over hydration is not generally a problem in
animals with normal kidney function. A recovering animal should be
watched continuously until in sternal recumbency, and able to move
around without plugging its nostrils with bedding. Some rodents left
overnight on pads or paper bedding will eat that bedding. To prevent
cannibalism, house rodents individually until they are ambulatory.
Postsurgical observations include a minimum daily observation of the
condition of the animal and the surgical site. A sample "Postoperative
Evaluation Record" is provided. Sutures (see attached Table 5 for data
on suture types and uses) and/or staples need to be removed 7-10 days
following surgery, if the rodent has not already done so. Any foreign
substance left in the incision for a long period of time serves as a
nidus of irritation and infection. A veterinarian should examine
incisions that do not appear to be healing.
Please identify cages with postoperative animals to:
*
explain the condition of the animals to animal care staff (e.g.
sedated animals thought to be ill)
*
assure animal care staff, veterinary staff, inspectors, and others
that proper care is being given to the animals,
*
inform animal care and veterinary staff how recently the
investigator has seen the animal to avoid contacting the
investigator to inform them of the animal’s condition.
Important techniques that are difficult to perfect include:
*
Touch only "prepped" areas with sterile instruments and gloved
hands.
*
Keep operating fields draped.
*
Do not let catheters or implants become contaminated.
*
Use sterile solutions.
*
Disinfect the tops of containers of solutions.
*
Use sterile technique to access implanted catheters.
Not only are the above recommendations more humane to our animal
charges, but following these recommendations will improve one’s
research by providing a less stressed animal and thereby decreasing
the number of variables in a research protocol. The rat has always
been considered "hardy" and not subject to postsurgical infections,
but published research has documented that postsurgical infections in
rats are subtle. The rat appears to eat and act normally, but will not
respond appropriately to research stimuli. As with all new and
improved techniques, patience and practice are required to harvest
full benefits from the use of aseptic surgical techniques in rodents.
There is ample literature available supporting the recommendations
presented in this document. Please contact one of the Department’s
veterinarians (x2017) for assistance or to provide referrals to other
researchers with applicable knowledge or skills.
Bibliography
Bojrab, MJ. 1990. Current Techniques in Small Animal Surgery. Lea and
Febiger, Philadelphia.
Bradfield, JF; Schachtman, TR; McLaughlin, RM; Steffan, EK. 1992.
Behavioral and Physiologic Effects of Inapparent Wound Infection in
Rats. Laboratory Animal Science 42(6): 572-578.
unliffe-Beamer, TL. 1993. Applying Principles of Aseptic Surgery to
Rodents. AWIC Newsletter 4(2) 3-6.
Elek, SD; Conen, PE. The Virulence of Staphlococcus pyogenes for Man.
A Study of the Problems of Wound Infection. 1957. British Journal of
Experimental Pathology 38: 573-583.
Gardiner, TW; Toth, LA. 1999. Stereotactic Surgery and Long-Term
Maintenance of Cranial Implants in Research Animals. Contemporary
Topics 38(1): 56-63.
Holman, JM; Saba, TM. 1988. Effect of Bacterial Sepsis on
Gluconeogenic Capacity in the Rat. Journal of Surgical Research 45:
167-175.
Maki, DG; Ringer, M; Alvarado, CJ. 1991. Prospective Randomised Trial
of Povidone-Iodine, Alcohol, and Chlorhexidine for Prevention of
Infection Associated with Central Venous and Arterial Catheter. The
Lancet 338: 339-343.
National Research Council. 1996. Guide for the Care and Use of
Laboratory Animals.
Pollari, FL; et al. 1996. Postoperative Complications of Elective
Surgeries in Dogs and Cats Determined by Examining Electronic and
Paper Medical Records. Journal of the American Veterinary Medical
Association 208(11): 1882-1886.
Popp, MB; Brennan, MF. 1981. Long-Term Vascular Access in the Rat:
Importance of Asepsis. American Journal of Physiology H606-H612.
Omatowski, J. 1989. Prevention and Control of Surgical Wound
Infection. Journal of the American Veterinary Medical Association
194(1): 107-113.
Sharp, PE; La Regina MC. 1998. The Laboratory Rat. CRC Press, Boca
Raton, FL.
Ulphani, JS; Rupp, ME. 1999. Model of Staphlococcus aureus Central
Venous Catheter-Associated Infection in Rats. Laboratory Animal
Science 49(3): 283-287.
Varma, S; Lumb WV; Johnson LW; Ferguson, HL. 1981. Further Studies
with Polyglycolic Acid (Dexon) and Other Sutures in Infected
Experimental Wounds. American Journal of Veterinary Research 42(4):
571-574.
Van Winkle, Jr., Walton; Hastings, JC. Considerations in the Choice of
Suture Material for Various Tissues. Surgery, Gynecology, and
Obstetrics 135:113-126.
 DEVELOPMENTAL REVIEWS OVERVIEW THE PURPOSE OF THE DEVELOPMENTAL REVIEW
DEVELOPMENTAL REVIEWS OVERVIEW THE PURPOSE OF THE DEVELOPMENTAL REVIEW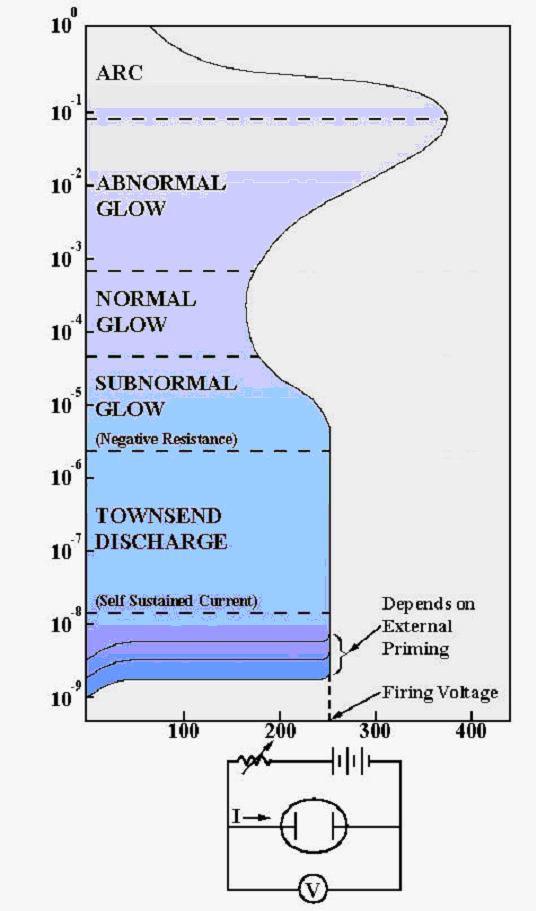 MODULE 7 PLASMA DISPLAYS 71 INTRODUCTION THE REALIZATION OF
MODULE 7 PLASMA DISPLAYS 71 INTRODUCTION THE REALIZATION OF Notice-of-Appointment-of-Election-Agents-Hillside
Notice-of-Appointment-of-Election-Agents-Hillside “AGRICULTURE PRODUCTIVITY ENHANCEMENT PROJECT BAS BOEN” TENDER NOTICE FOR
“AGRICULTURE PRODUCTIVITY ENHANCEMENT PROJECT BAS BOEN” TENDER NOTICE FOR WWWJUSTICEGOVUK 91034 JUNE 2014 FREEDOM OF INFORMATION REQUEST YOU
WWWJUSTICEGOVUK 91034 JUNE 2014 FREEDOM OF INFORMATION REQUEST YOU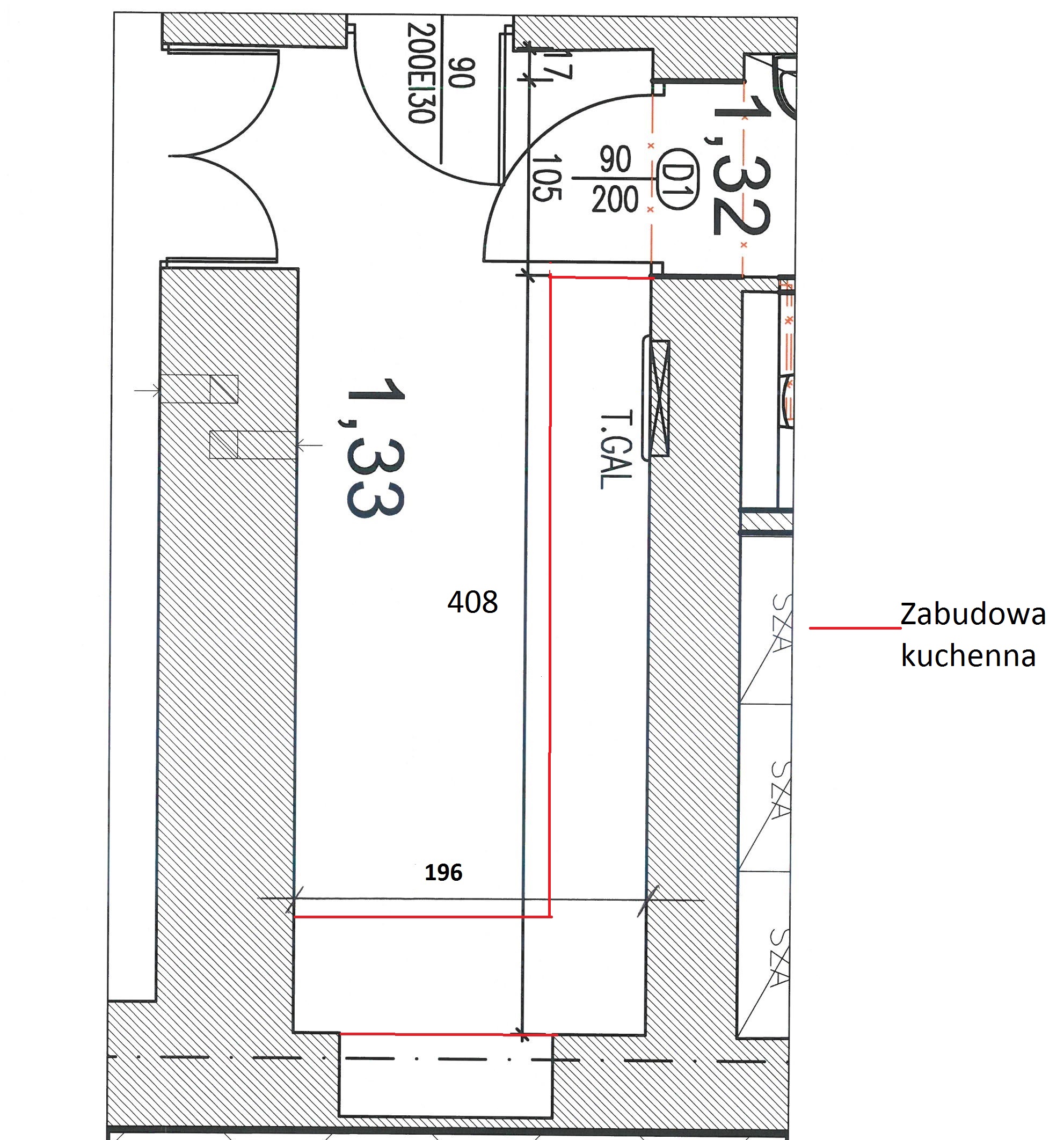 OPIS PRZEDMIOTU ZAMÓWIENIA CZĘŚĆ II ZAMÓWIENIE DOTYCZY WYKONANIA I
OPIS PRZEDMIOTU ZAMÓWIENIA CZĘŚĆ II ZAMÓWIENIE DOTYCZY WYKONANIA I PROJECT NAME DISPOSITION PLAN VERSION TYPE VERSION DATE
PROJECT NAME DISPOSITION PLAN VERSION TYPE VERSION DATE NOTA SOBRE LOS ASPECTOS DE DISCAPACIDAD DE LA RESOLUCIÓN
NOTA SOBRE LOS ASPECTOS DE DISCAPACIDAD DE LA RESOLUCIÓN MARYLAND SOCIAL EMOTIONAL FOUNDATIONS FOR EARLY LEARNING PYRAMID MODEL
MARYLAND SOCIAL EMOTIONAL FOUNDATIONS FOR EARLY LEARNING PYRAMID MODEL AGIRI HAU BABESTUTA DAGO MARKATUTA DAUDEN ESPAZIOETAN BAINO EZIN
AGIRI HAU BABESTUTA DAGO MARKATUTA DAUDEN ESPAZIOETAN BAINO EZIN EPISODE RECORD FOR………………………DATE OF BIRTH………… THIS FORM IS TO
EPISODE RECORD FOR………………………DATE OF BIRTH………… THIS FORM IS TO